PulmoRehab goals
The goal is to reduce social inequalities in health by providing remote access to health services through a personalized care system for patients with lung diseases. The system will include remote monitoring and tele-rehabilitation based on Artificial Intelligence methods.
The project will contribute to the program’s outcome by piloting the provision of a telemonitoring and telerehabilitation system to a gender- and location-diverse group of patients, which will mimic the methods and procedures of hospital-based respiratory monitoring and rehabilitation routinely used (4-group Szczegielniak’s system).
Benefits of tele-rehabilitation
Defining monitoring programs with full bio-feedback (12 patient vital function signals and application – all diagnostic tests and breathing exercises),
Implementation of observation plans in the patient application
Creation of games simulating stationary exercises (visualization on the application that the patient is in the oxygen area of the exercise, measurement of airflow with feedback – maintenance of the respiratory rhythm set in the simulation – spirometry, bioimpedance and accelerometry)
 Consortium:
Consortium:
Leader: SP ZOZ MSWiA Specialized Hospital in Głuchołazy named after St. John Paul II.
Technical management of the project: Prof. Jan Szczegielniak
Technology partner: AIDMED
The beneficiary of the project is the St. John Paul II SP ZOZ MSWiA Specialized Hospital in Glucholazy, which together with 10 partners will implement a project that aims to reduce social inequalities in health care by providing remote access to health services through a personalized care project for patients with Chronic Obstructive Pulmonary Disease. The system will include remote monitoring and tele-rehabilitation based on Artificial Intelligence methods.
PulmoRehab observation details
The observation card consists of: Recording of biosignals (spirometry, ECG, saturation, respiration-method of changes in chest impedance and nasal airflow, body movements, chest movements, ambient acoustics-cough and skin temperature), directly and during teleconsultation-clinical history, information about the course of the disease and rehabilitation, assessment of quality of life and motivation (other socio-demographic questionnaires, dimensions of anxiety and depression, (e-)health competence, satisfaction with the use of the tool), etc.
Remote diagnosis, screening for the most common comorbidities like sleep apnea, arrhythmia, etc. Sleep-disordered breathing is one of the diseases that can accompany respiratory diseases – hence screening patients will be subjected to remote diagnosis.
Adaptation of a system to detect sudden exacerbation of respiratory symptoms based on Artificial Intelligence methods – including the generation of alarms
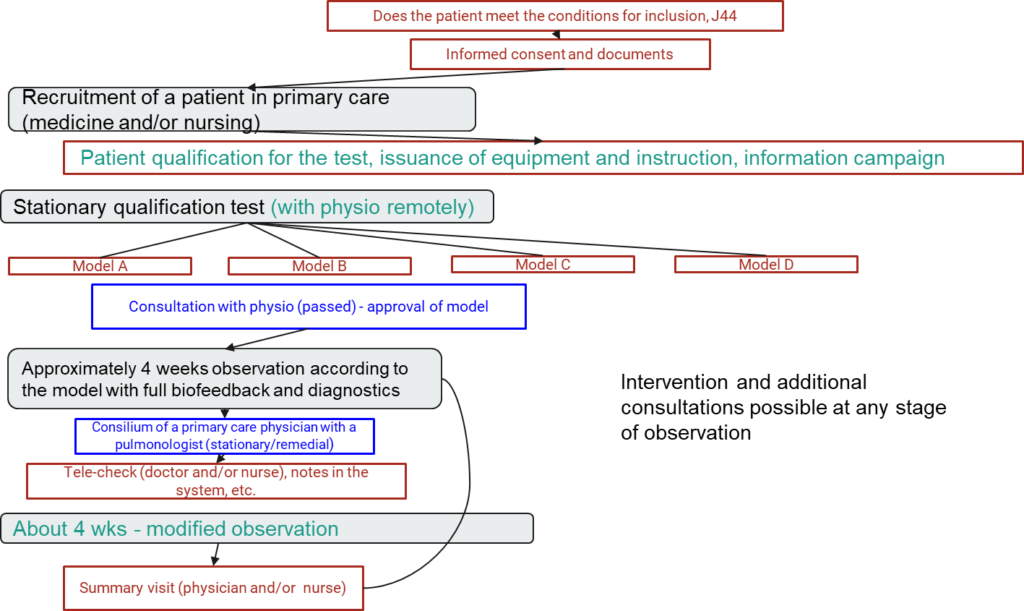
PulmoRehab study details
- Pilot of a telemedicine system to support teleobservation and telerehabilitation of pulmonary (COPD) patients; Implementation of the rehabilitation program at home; Increased availability of medical services: access to rehabilitation programs, access to specialists in medical and rehabilitation areas; rural and small town orientation; cost reduction; Coordination of various specialists
- ~500 patients, ~2 months of telerehabilitation
- 2 teleconsultations with pulmonologists, teleobservation and teleconsultations with physiotherapists,
- Symptom questionnaires, remote recording of biosignals, remote testing
PulmoRehab hypothesis
The primary endpoint of the prospective cohort study will be to compare the change in performance characteristics of patients (before/during/after) submodels with patients (after normalization following control variables) with patients participating only in inpatient/ambulatory rehabilitation.
The secondary endpoints of the prospective cohort study will be: Cost estimates (technology, staff labor share) of each cohort Variation in satisfaction with system use and subjective quality of life between cohorts.
Our research hypothesis is that there will be subjective and objective improvements in respiratory/general fitness in patients undergoing tele-rehabilitation, and that there will be no clear significant difference relative to the baseline of inpatient/ambulatory rehabilitation. This will allow us to analyze the cost-effectiveness of the proposed cohorts relative to the baseline.
Project financed by:
– Norwegian Ministry of Foreign Affairs in the amount of PLN 2,606,894.72;
– State budget in the amount of PLN 460,040.28.
Completion date: 31.12.2023, Project value: PLN 3,066,935.00
